セカンドオピニオンから ペットロスまで どうぶつよろず相談



https://ja.wikipedia.org/wiki/ネズミ
https://en.wikipedia.org/wiki/Dipodidae
https://en.wikipedia.org/wiki/Caviidae
https://ja.wikipedia.org/wiki/テンジクネズミ科
https://ja.wikipedia.org/wiki/カピバラ
https://en.wikipedia.org/wiki/Capybara
https://en.wikipedia.org/wiki/Hydrochoerus
https://en.wikipedia.org/wiki/Lesser_capybara
 |
 |
|
羽ばたきロコモーション 海鳥132021年8月20日 KVC Tokyo 院長 藤野 健です。 カピバラと他の水棲齧歯類との運動特性の比較をこれまで行ってきました。最終的にビーバーの尻尾の扁平化の持つ機能的意義について考察しようと思いますが、その前に途中追加的にロコモーション関連の話をまた~りと採り上げます。運動性に関することですので、youtube からの動画資料を多くお借りしての解説です。 ウミガメの様な水中羽ばたき型の遊泳ロコモーションを示す各種の動物を引き続き見て行きましょう。飛べないウであるガラハゴスコバネウがなぜ飛べなくなったのかを引き続き考えます。ガラパゴスコバネウの翼の退縮が、極めて稀な疾患としてヒトに見られるセンセンブレンナー症候群の原因遺伝子と同じ遺伝子の異常に関連している、との Kruglyak 氏のグループの論文を前々回、前回と紹介しました。今回は、真逆の視点から、即ち、このセンセンブレンナー症候群の実状からこの論文を批判的に吟味していきましょう。まぁ、久しぶりの医学的なお話になります。 以下本コラム作成の為の参考サイト:https://ja.wikipedia.org/wiki/ウ科https://en.wikipedia.org/wiki/Cormoranthttps://en.wikipedia.org/wiki/Flightless_cormoranthttps://ja.wikipedia.org/wiki/ガラパゴスコバネウhttps://science.sciencemag.org/content/356/6341/eaal3345.fullA genetic signature of the evolution of loss of flight in theGalapagos cormorantAlejandro Burga, Weiguang Wang, Eyal Ben-David, Paul C. Wolf, Andrew M. Ramey, ClaudioVerdugo, Karen Lyons, Patricia G. Parker, Leonid KruglyakScience 02 Jun 2017: Vol. 356, Issue 6341, eaal3345, DOI:10.1126/science.aal3345(全文無料で読めます)https://www.sciencemag.org/news/2017/06/how-clumsy-galapagos-cormorant-lost-its-flightHow the clumsy Galapagos cormorant lost its flight, ByRyan CrossJun. 1, 2017doi:10.1126/science.aan6921(全文無料で読めます)https://en.wikipedia.org/wiki/Sensenbrenner_syndromehttps://kenkojiten.com/sensenbrenner-syndrome-causes-symptoms-treatment/センセンブレナー症候群:原因、症状、治療https://www.jst.go.jp/pr/announce/20100125/index.html体の左右非対称性をもたらす繊毛の回転運動、その仕組みを解明 |
||
 |
 |
Cute Little Girl Suffers From Rare Disease 2016/08/30 SWNS
A cute seven-year-old girl is one of just 20 people in the WORLD suffering from a
disease which is so rare that it took doctors THREE years to diagnose her.Matilda
Hatton suffers from Sensenbrenner Syndrome which causes her to have morphic
facial features and shorter limbs. The youngster grows at a slower rate than other
children because of the ultra-rare multi-system disorder. She was born with just 30
percent kidney functions and her liver was also abnormal. Incredibly, thedisease is
so rare that Matilda wasn't diagnosed until she was three-years-old because
doctors were baffled by the symptoms. https://youtu.be/IVF39uZvpX8
7歳の少女が世界で20人しか居ない稀な病気に罹患し診断が付くまで3年も掛かりました。
マチルダ・ハットンはセンセンブレンナー症候群に苦しんでいますが彼女に特徴的な顔面形状、
短い四肢をもたらしています。他の子供達より成長が遅いのですがこれは非常に稀な多系統
の障害のゆえです。彼女は僅か30%しか機能しない腎臓を持って生まれ、また肝臓も正常で
は無かったのです。信じられないことですが、この病気は稀なのでマチルダが3歳になるまで
診断が付きませんでした。医者が症状に当惑したからです。
臓器不全に対しては対象療法的にケアしていくしかありませんが、この子が元気に成長して
くれることを願うばかりです。
|
|
|
センセンブレンナー症候群英語版 Wikipedia の本疾患の記事が専門用語の羅列であり、解説記事としてのデキが悪い、いや、まだ記事としての体を為していないと感じますが、現時点では日本語版の記事も無いので、まずは一応和訳しながら解説を加えて行きましょう。https://en.wikipedia.org/wiki/Sensenbrenner_syndromeから引用:Wikipedia contributors, "Sensenbrenner syndrome," Wikipedia, The Free Encyclopedia, https://en.wikipedia.org/w/index.php?title=Sensenbrenner_syndrome&oldid=1013733763 (accessed August16, 2021).(以下原文の一部)Sensenbrenner syndromeOther names Cranioectodermal dysplasiaSensenbrenner syndrome (OMIM #218330) is a rare (less than 20 cases reported by 2010)multisystem disease first described by Judith A. Sensenbrenner in 1975.It is inherited in anautosomal recessive fashion, and a number of genes appear to be responsible. Three genesresponsible have been identified: intraflagellar transport (IFT)122 (WDR10), IFT43- a subunit ofthe IFT complex A machinery of primary cilia, and WDR35 (IFT121: TULP4). It is also known asSensenbrenner-Dorst-Owens syndrome, Levin syndrome I and cranioectodermal dysplasia (CED)PresentationThese are pleomorphic and includedolichocephaly (with or without sagittal suture synostosis), microcephaly, pre- and postnatalgrowth retardation, brachydactyly, narrow thorax, rhizomelic dwarfism, epicanthal folds,hypodontia and/or microdontia, sparse, slow-growing, hyperpigmented, fine hair, nail dysplasia,hypohydrosis, chronic kidney failure, heart defects, liver fibrosis, visual deficits, photophobia,hypoplasia of the posterior corpus callosum, aberrant calcium homeostasisElectroretinography shows gross abnormalities.Two fetuses of 19 and 23 weeks gestation have also been reported. They showed acromesomelicshortening, craniofacial characteristics with absence of craniosynostosis, small kidneys withtubular and glomerular microscopic cysts, persistent ductal plate with portal fibrosis in the liver,small adrenals, an enlarged cisterna magna and a posterior fossa cyst.CauseThe gene IFT122 is located on the long arm of chromosome 3 (3q21-3q24). The gene lies on theWatson (plus) strand and is 80,047 bases in length. The encoded protein has 1241 amino acidsand a predicted weight of 141.825 kiloDaltons (kDa). It is a member of the WD repeat proteinfamily. WDR35 is also a member of the WD repeat protein family. The gene is located on the shortarm of chromosome 2 (2p24.1-2p24.3) The gene lies on the Crick (minus) strand and is 79,745bases in length. The encoded protein is 1181 amino acids in length and its predicted molecularweight is 133.547 kiloDaltons. The gene IFT43 lies on the Watson (plus) strand of the long arm ofchromosome 14 (14q24.3). A mouse model for IFT122 has been created. Mutants deficient inIFT122 show multiple developmental defects (many are lethal), including exencephaly, situsviscerum inversus, delay in turning, hemorrhage and defects in limb development. In the node,primary cilia were absent or malformed in homozygous mutant and heterozygous embryos,respectively. Impairment of the Sonic hedgehog pathway was apparent in both neural tubepatterning (expansion of motoneurons and rostrocaudal level-dependent contraction or expansionof the dorsolateral interneurons) and limb patterning (ectrosyndactyly).PathophysiologyThe IFT machinery is organized in two structural complexes - A and B. These complexs areinvolved in the coordinated movement of macromolecular cargo from the basal body alongaxonemal microtubules to the cilium tip and back again. The anterograde movement of IFTparticles out to the distal tip of cilia and flagella is driven by kinesin-2 while the retrogrademovement of particles back to the cell body is driven by cytoplasmic dynein 1b/2. The IFT-Aprotein complex is involved in retrograde ciliary transport. Disruption of IFT43 disturbs transportfrom the ciliary tip to the base. Anterograde transport in the opposite direction remains normalresulting in accumulation of the IFT complex B proteins in the ciliary tip.PathologyThe visual defects are due to photoreceptor dystrophy. The chronic kidney failure is due totubulointerstitial nephropathy. The liver fibrosis is secondary to ductal plate malformation. |
||
|
|
Exome Sequencing Identifies WDR35 Variants Involved in Sensenbrenner Syndrome
Christian Gilissen, et al. The American Journal of Human Genetics 87, 418-423,
September 10, 2 in Accelerating Scientific Discovery Sure Select Publication
Compendium January 2011, pp.13-18
https://www.researchgate.net/profile/Arcangela-Iuso/publication/47701349/figure/
fig5/AS:667094156861445@1536059049131/Two-Patients-with-Sensenbrenner
-Syndrome-for-Whom-Exome-Sequencing-Was-Performed-A.ppm
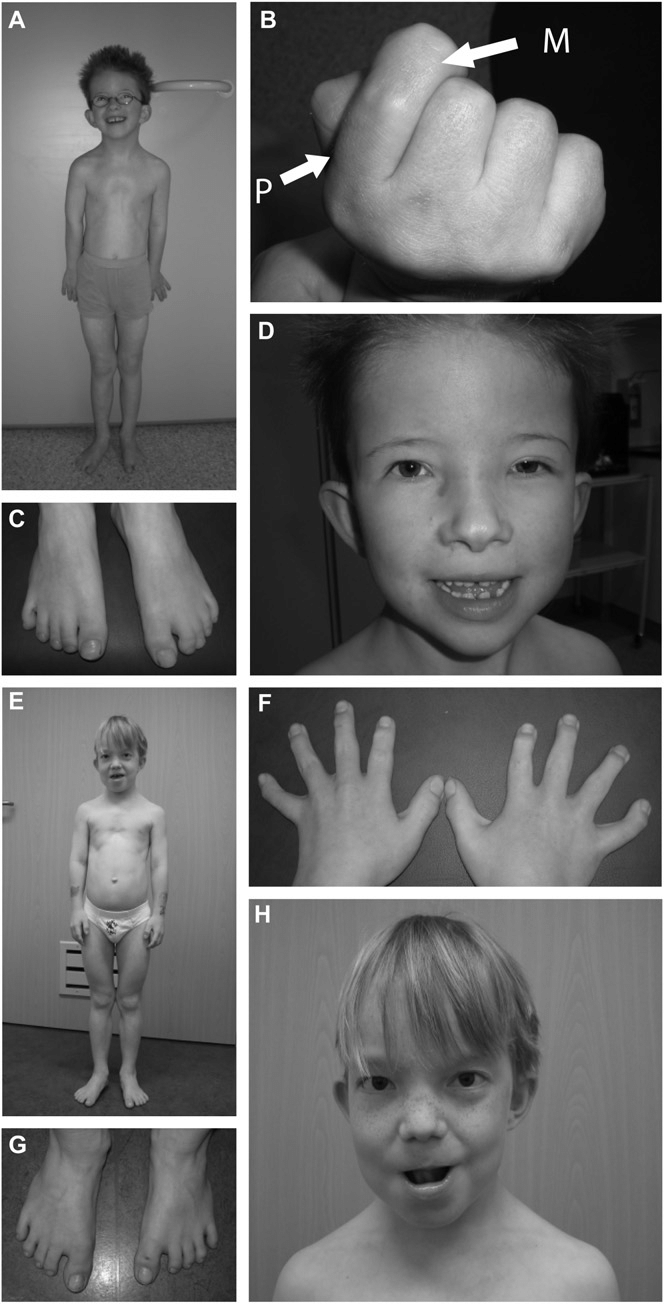
Two Patients with Sensenbrenner Syndrome for Whom Exome Sequencing Was
Performed (A) Patient 1: small thorax, pectus excavatum, rhizomelic shortening
of limbs. (B) Shortening of proximal second phalanx. The proximal phalanx is
indicated by ''P''; the middle phalanx is indicated by ''M.'' (C) Syndactyly 2-3 right
foot, 2-3-4 left foot. (D) Hypertelorism, unilateral ptosis of left eye, low-set ears,
everted lower lip. (E) Patient 2: small thorax, pectus excavatum, rhizomelic
shortening of limbs. (F) Short, broad hands. (G) Bilateral sandal gap between
first and second toe. (H) Hypertelorism, low-set simple ears, thin hair.
エクソームシーケンシングが行われたセンセンブレンナー症候群の2患者
患者1では、図A:小胸郭、漏斗胸、四肢の近位側短縮、図B:人差し指の基節骨Pの
短縮、図C:右足第2,3趾、左足第2,3,4趾の合趾、図D:両眼隔離、片側眼瞼下垂、
耳介低位、下口唇反転、患者2では、図E:小胸郭、漏斗胸、四肢の近位側短縮、図F:
短く幅の広い手、図G:第1,2趾間の左右両側性の乖離、図H:両眼隔離、
単純な造りの耳介の低位、薄い毛髪。
胸郭の発達が弱く、肩幅が狭いことが歴然としています。上腕骨と大腿骨が短いですね。
|
|
|
センセンブレンナー症候群別名頭蓋外胚葉異形成症センセンブレンナー症候群 (OMIM#218330) は、Judith A. Sensenbrenner (ジュディス A. センセンブレンナー)が 1975年に最初に記載した稀な (2010年までの報告で20症例以下) 多系統疾患である。常染色体劣性形式で遺伝し、幾つかの遺伝子がそれに関与する様に見え、これまでに3つの責任遺伝子が同定されて来ている。これらは、繊毛内タンパク質輸送遺伝子 (IFT)122 (WDR10)、IFT43遺伝子 - これはIFT複合体A 一次繊毛装置のサブユニット、それとWDR35 (IFT121: TULP4) 遺伝子である。本疾患はセンセンブレンナー-ドルスト-オーウェンス症候群、レビン症候群 1、また頭蓋外胚葉異形成症 (cranioectodermal dysplasia, CED) としても知られる。症状本疾患は多形性を示し以下の症状を含む:長頭症(矢状縫合癒合症の有り無し)、小頭症、出生前後の成長遅延、短指症、胸郭狭窄、近位点型小人症(=上腕骨と大腿骨の短縮型小人症)、内眼角贅皮、歯数不足及び或いは矮小歯、疎で成長の遅い色素過剰の細い毛髪、爪の異形成、乏汗症、慢性腎不全、心不全、肝線維症、視覚障害、羞明、脳梁後部の低形成、カルシウム恒常性の異常網膜電図像は肉眼的な異常所見を示す。妊娠19週並びに23週齢の胎児2体も報告されているが、四肢先端中部骨格短縮、頭蓋骨縫合早期癒合症を欠く特徴的な頭蓋顔面、尿細管及び糸球体の微小嚢胞を伴う矮小腎、肝臓内の門脈線維症を伴う持続性胆管板、小副腎、大脳大槽の拡大及び後頭蓋嚢胞を示した。原因遺伝子IFT122は、3番染色体の長腕上に位置している (3Q21-3Q24)。この遺伝子はワトソン(プラス)鎖上にあり、長さは80,047塩基である。コードされたタンパク質は1241個のアミノ酸を持ち予測重量は141.825キロダルトン(KDA)である。このタンパク質はWDRタンパク質ファミリーの一員である。WDR35 もまたWDRタンパク質ファミリーの員である。遺伝子は第2染色体の短腕 (2P24.1≦2P24.3)上に位置しており、遺伝子は Crick(マイナス)鎖上にあり、長さが79,745塩基である。コードされたタンパク質は1181個のアミノ酸長を持ち、その予測分子量は133.547キロダルトンである。遺伝子IFT43 は、第14染色体の長腕のワトソン(プラス)鎖にある (14q24.3)。IFT122のマウスモデルが作出されている。は、IFT122を欠く突然変異個体は、多系統の発達障害を示し(多くは致死的)、これは外脳症、内臓逆位、旋回遅延、出血、及び四肢発達障害を含む。ノード(受精後7.5日頃のマウス胚は、体の中心部、腹側表面に「ノード」と呼ばれる窪んだ構造を一時的に作るが、ノードを構成する数百の細胞には繊毛(ノード繊毛)が生えていて、この繊毛が回転運動することにより左向きの水流がながれ、細胞の対称性を破り臓器が正しく形成されると考えられている)中に於いては、一次繊毛はホモ接合の突然変異体には欠損し、またヘテロ接合の胚ではその形態発生異常を来した。ソニックヘッジホッグシグナル伝達経路の障害は、神経管パターニング(運動ニューロンの拡大と背外側介在ニューロンの体軸前後方向のレベル依存性の収縮或いは拡大)並びに四肢パターニング(無指合指症)の両者に於いて明らかであった。病態生理学繊毛内タンパク質輸送装置 (IFT machinery) は2つの構造複合体 A, Bで編成されている。 これらの複合体は、軸腔内微小管に沿う基部から繊毛の遠位端への、またその逆方向の、高分子輸送の協調運動に関与している。IFT粒子の繊毛並びに鞭毛の遠位端への前向的な動きはキネシン-2によって駆動されるが、一方、粒子が細胞体に戻る逆行的な運動は細胞質ダイニン1B / 2によって駆動される。IFT-Aタンパク複合体は逆行性の繊毛輸送に関与している。 IFT43 の破壊は繊毛の端から基部への輸送を妨害する。 これと逆方向の前向性の輸送は正常なままであり、結果として繊毛先端のIFT複合Bタンパク質の蓄積をもたらす。病理学視覚障害は光受容体ジストロフィーに拠るものである。 慢性腎不全は尿細管間質性腎症に拠る。肝線維症は胆管板奇形に続発する。(以上院長和訳)*外見的に目立つところとして頭蓋骨の異常、左右幅の狭い胸郭、四肢骨近位の短縮、指の短縮などの奇形が挙げられますが、臓器の形成不全や目の異常など多々の臨床像が観察されます。 *端的に言えば、細胞と細胞の正しい信号の遣り取りに利用される繊毛の異常、機能不全が生じ、正しい発達、成長が阻害されるとの疾患です。多くは致死的で出産に至りませんが、挙子され得た者はまだ軽い症状であると言えるのかも知れません。但し、臓器障害などに拠り早世する可能性はあります。 *しかしながら、ガラパゴスコバネウでは翼が短い以外の特徴以外は特に見られず、別段<病気>ではありませんし、後肢の大腿骨が短縮も示さず、寧ろ強大に発達していて潜水に利するぐらいです。翼の骨も上腕骨が特に短縮していることはなく、翼を構成する前肢骨全体が等しいプロボーションのままに縮んでいる様に見えます(前回コラムの図参照)。生まれた全ての個体で翼が短いので、常染色体劣性遺伝形式ではなく、翼を短くする遺伝子はホモ接合体の筈ですが、これが為に一段と強い病理像を呈することもありません。仮に臓器障害があれば強負荷運動である潜水などはとても出来ないでしょう。 *以上から判断すると、ガラパゴスコバネウの翼の退縮は、ヒトのセンセンブレンナー症候群とはだいぶ趣を異にしていることが分かります。他に同様の遺伝子の異常が見付かったにしても、どうして翼のみにその様な形態変化が起きるのかを解明しない限り、1つの仮説の域を出ない、と院長は感じました。 *翼の発達時のみ遺伝子が作動するが、他の部位には異常を起こさずに動きが抑制される、などの(都合の良すぎる!)補償的な遺伝的機序が働く可能性も考えられますが、謎だらけですね。実は発見された遺伝子の異常は無関係であり、全く別の機序で短縮した翼が形成される可能性も捨てられません。即ち、ニワトリが飛翔力をほぼ失ったのと同じ様な進化の理由が作動した可能性です。フクロウオウムのカカポやヤンバルクイナなどを含め、翼が退縮することに関与する共通の遺伝的な変異が、全く別個に存在する可能性もあります。もしそれが証明し得ればノーベル医学生理学賞が貰えるかも知れません。皆さんはどうお考えでしょうか? ガラパゴスコバネウの項は今回で終わり、次回からはまた別の海鳥のお話に入ります。飛べなくなった-これはロコモーション上の重大な変化になります-トリに関しては後日纏めて別コラムを仕立てる予定です。 |
||
|
|